The thoracic region consists of 12 vertebrae, and is the largest
segment of the spine. Due to its articulations with rib cage, the
thoracic spine is more rigid than the cervical and lumbar regions. It
protects thoracic viscera such as heart, lungs, and great vessels.
Starting from early fetal period, the sagittal alignment of the
thoracic spine is kyphotic, ranging between 20 to 40 degrees in adults.
BONY ANATOMY
The thoracic vertebrae are intermediate in size between the cervical
and lumbar vertebrae. There are regional variations from Tl to T12. Tl
shows some similarities to the cervical vertebrae with uncinate
processes protruding from its superolateral edges. T2 to T8 are quite
uniform, and are considered as typical thoracic vertebrae. T9 to T12
are the transition vertebrae, and shows some similarities with lumbar
vertebrae. Thoracic region can also be subdivided as upper (T1-T4),
middle (T5-T8), and lower (T9-T12) thoracic areas.
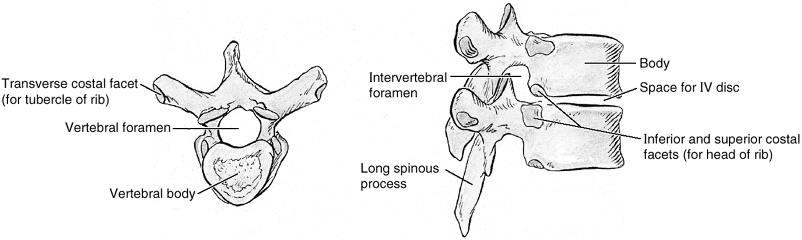
Vertebral bodies: Thoracic vertebral
bodies are heart-shaped, with a deeper anterior posterior dimension
than medio-lateral width. The left side of the vertebral body may be
slightly flattened or depressed due to pulsations of the aorta. The
dimensions of the bodies increase as one moves down the spinal column
(see picture).
Pedicles: The pedicles connect the
vertebral bodies to the posterior elements. They are cylinder-like
structures and their medial cortex is thicker than the lateral cortex.
They are oval in cross section, having larger heights and smaller
widths. However, their elliptical shapes are highly variable.
The medial wall of the pedicle is bounded by the exiting nerve roots
and the thecal sac. Laterally the pedicle is bounded by the
costovertebral ligaments, joints, and ribs. Superiorly and inferiorly,
the pedicles are bounded by the adjacent neural foramen. Pedicle sizes
are around 6 to 8 mm from T1 to T12. The smallest sizes of pedicles are
found between T3 and T6 and may only be 10 mm in height and 4 mm in
width. The largest pedicle diameter is usually in the low thoracic
region, being 14 mm in height and 8 mm in height at T12 level. In the
proximal thoracic spine, pedicle sizes are slightly larger than those
of middle thoracic levels. Pedicle axes show convergence at the axial
(transverse) plane. These transverse angles are also show regional
differences. The largest transverse angulations are observed at T1 (30
degrees). A steady reduction in transverse angulations is observed as
one moves caudally, with the transverse inclination of the T12 pedicles
being approximately 0 degrees. The pedicles are also show downward
inclination at the sagittal plane. This inclination is at the posterior
superior to anterior inferior direction, and is around 20
degrees.Determining
the posterior projection of the pedicle on the posterior elements is of
crucial importance during pedicle screw placement. The center of the
pedicle projection lies at the intersection of a line drawn parallel to
the edge of the transverse process in its superior one-third, and a
line drawn 1 to 2 mm medial to the lateral edge of the lamina.
Facet Joints: The thoracic facets
oriented in the coronal plane. Thus, thoracic facets allow primarily
lateral bending and axial rotation. The superior articular facet of the
caudal vertebrae forms the roof of the neural foramen.
Transverse Processes: The transverse
processes join the pedicles and the laminae at their bases. They extend
lateral and posterior, to make room for the ribs to pass anterior to
them. They articulate with the ribs on their anterolateral surface. T1
transverse processes is the largest and then gradually decrease in size
toward T12. The angulation in the transverse plane changes from fairly
flat at T1 to more posteriorly protruding at T12.
Lamina and Spinous Processes: The
thoracic vertebrae typically have long, slender spinous processes that
point downward and overlap vertebral arches of the vertebra below.
Thus, thoracic laminectomy requires removal of the inferior portion of
the rostral spinous process. Both the laminae and the spinous processes
slope in a superior anterior to posterior inferior direction. They
serve as attachment points for the segmental spinal muscles and the
thoracolumbar fascia.
RIB CAGE
Each thoracic segment is accompanied by a pair of ribs. The
ribs articulate with the spinal column posteriorly, and the sternum
anteriorly. Ribs 1 to 7 are termed as true ribs. They articulate with
the sternum directly. Ribs 8-10 are termed as false ribs, and they
articulate with the costocartilage of the rib above. Ribs 11 and 12 are
termed as floating ribs, because they do not articulate to either the
sternum or the costal cartilage at their distal ends (see picture).
Costovertebral Joints (Costal facets):
The first, eleventh, and twelfth pair of ribs articulate with their
named vertebra only. The second through tenth ribs articulate both with
their named vertebral body and with the intervertebral disk and the
vertebra above. Also, each pair of ribs articulates with the anterior
surface of the transverse process of its named vertebrae. The ribs are
connected to the vertebral column by the costovertebral ligaments. The
space between the transverse process, the lateral edge of the pedicle,
and the medial edge of the rib constitutes a triangular
osteoligamentous zone. This zone can be used for extrapedicular screw
placement (see picture).
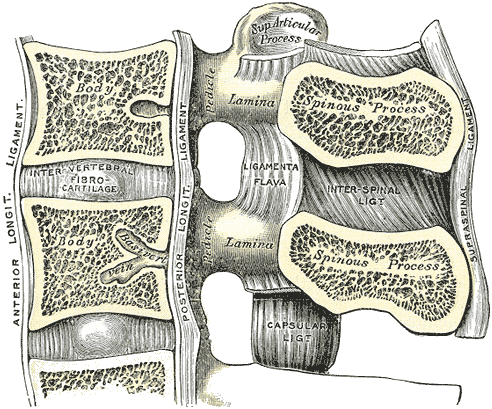
LIGAMENTS
The functions of the ligaments are to allow and limit physiologic
motion, to contribute to the spinal stability, and to protect the
spinal cord in trauma. There are seven spinal ligaments (see picture).
Anterior Longitudinal Ligament: The
anterior longitudinal ligament (ALL) runs down the ventral surface of
the spine from the occiput to the sacrum. The ALL is thicker and
narrower in the thoracic region. The ligament is thick and slightly
more narrow over the vertebral bodies and firmly attached to the edges
of the vertebral bodies. On contrary, the ALL thinner but slightly
wider over the intervertebral discs and it is loosely attached to the
disk annulus. The ligament has three layers: superficial, intermediate
and deep. The superficial layer traverses three or four vertebrae, the
intermediate layer covers two or three and the deep layer is only
between individual vertebrae. The deep layers of the ligament, as it
crosses the vertebral body, blend with the periosteum.
Posterior Longitudinal Ligament: The
posterior longitudinal ligament (PLL) is situated within the vertebral
canal. It arises from the posterior aspect of the basiocciput, is
continuous with the membrana tectoria, and runs over the posterior
surfaces of the bodies of the vertebrae, down to the coccyx. It is
wider over the intervertebral disk than over the vertebral body. This
is important in understanding the typical location for a disc
herniation. The PLL is composed of smooth, shining, longitudinal
fibers, denser and more compact than those of the ALL, and consists of
superficial layers occupying the interval between three or four
vertebae, and deeper layers which extend between adjacent vertebrae.
Intertransverse Ligaments: The
intertransverse ligaments are situated between the transverse
processes. In the thoracic region, they are rounded cords, and closely
connected with the deep muscles of the back.
Capsular Ligaments: In general, a
capsular ligament is a part of the articular capsule that surrounds a
synovial joint. In the spine, the capsular ligaments are attached to
the articular margins of the articular processes. The fibers are
oriented perpendicular to the facet joint and are stronger in the
thoracic and lumbar region than in the cervical region.
Ligamentum Flavum: The ligamentum
flavum connects the anteroinferior edge of the lamina to the
posterosuperior edge of the lamina below. They are best seen from the
interior of the vertebral canal. It extends from C2 to S1. The ligament
consists of two lateral portions which start out on either side of the
roots of the articular processes, and extend backward to the midline;
the posterior margins of the two portions are in contact and to a
certain extent united, there are small gaps for the passage of small
vessels. The ligamentum flavum is thicker in the thoracic region. This
ligament is composed mainly of elastic fibers, and that elasticity
serves to preserve the upright posture, and to assist the vertebral
column to resume after flexion. Hypertrophy of this ligament is one of
the major reasons of spinal stenosis.
Interspinous Ligaments: The
interspinous ligaments connect adjacent spinous processes, and runs
obliquely from the anterior inferior aspect of the spinous process
above to the posterior superior aspect of the spinous process below.
The ligament is thin and membranous, and narrow and elongated in the
thoracic region. They meet the ligamentum flavum in front and the
supraspinal ligament behind.
Supraspinous Ligament: The supraspinous
ligament is a strong fibrous cord, which connects together the tips of
the spinous processes from the C7 to the sacrum. In the cervical area,
it extends as the ligamentum nuchae. The supraspinous ligament consists
largely of tendinous fibers derived from the back muscles and is better
developed in the upper lumbar region and is often absent in the lower
lumbar region. The ligament closely blended with the neighboring
fascia. The most superficial fibers of this ligament extend over three
or four vertebrae; those more deeply seated pass between two or three
vertebrae while the deepest connect the spinous processes of
neighboring vertebrae. Between the spinous processes, it is continuous
with the interspinous ligament.
MUSCLES
Because most body weight lies anterior to the vertebral column, the
many strong muscles attached to the spinous and transverse processes
are necessary to support and move the vertebral column. Those muscles
and the complex neuromuscular controls is essential to provide spine
stability, and to produce balanced spinal motion during physiologic
activities. The spinal musculature does not only play an important role
in spine stability, motion, and balance; but also interrelate with the
upper and lower extremity function.
There are two major groups of muscles in the back. The extrinsic back
muscles produce and control limb and respiratory movements. The
intrinsic (deep) back muscles act on the vertebral column, maintaining
posture and producing its movements (see picture).
Extrinsic Back Muscles
The extrinsic back muscles include superficial and intermediate
muscles. The superficial extrinsic back muscles include trapezius,
latissimus dorsi,
levator scapulae, and rhomboids. The function of this muscle group is
to connect the upper limbs to the trunk and produce and control limb
movements. Although located in the back, these muscles receive their
nerve supply from the anterior rami of cervical nerves and act on the
upper limb. The trapezius receives its motor fibers from cranial nerve
XI, the spinal accessory nerve. The intermediate extrinsic back muscles
include serratus posterior superior and inferior. Those are thin,
superficial respiratory muscles. They are mostly described as muscles
of the thoracic wall, and innervated by intercostal nerves. The
serratus posterior superior lies deep to the rhomboids, and the
serratus posterior inferior lies deep to the latissimus dorsi.
Intrinsic Back Muscles
The intrinsic
back muscles (also called as deep back muscles, muscles of back proper)
are act to maintain posture and control movements of the vertebral
column, and innervated by the posterior rami of spinal nerves. The deep
muscles of the back are separated from the overlying muscles by fascia.
That fascia attaches medially to the nuchal ligament, the tips of the
spinous processes of the vertebrae, the supraspinous ligament, and the
median crest of the sacrum. It attaches laterally to the cervical and
lumbar transverse processes and to the angles of the ribs. The thoracic
and lumbar parts of the deep fascia constitute the thoracolumbar
fascia. In the thoracic region, the fascia over the muscles is thin,
attached in the midline to the spinous processes, and laterally, at the
edge of the muscles to the ribs and fascia, covering the intercostal
muscles.
These muscle groups can be differentiated by the direction of
their fibers. A distinction is also made on the length of the muscle
fibers, whether they attach to the ribs and also by the area of the
muscle—capitis, cervicis, thoracis, and lumborum.
The deep back muscles can be grouped into superficial, intermediate,
and deep layers
according to their proximity to the surface. There is also another
group, which can be classified as minor deep layer muscles. Superficial
layer of intrinsic back muscles include splenius capitis and cervicis
muscles. The splenii arise from the midline and extend superolaterally
to the cervical vertebrae (splenius cervicis) and cranium (splenius
capitis). The splenii cover and hold the deep neck muscles in position.
The splenius capitis arises from the ligamentum nuchae and the spinous
processes from C7 to T3 or T4 and attaches to the superior nuchal line
and mastoid process of the skull. The splenius capitis arises from the
spinous processes below the splenius capitis, usually T3 to T6.
Intermediate layer of intrinsic back muscles also known as erector
spinae muscles and include iliocostalis, longissimus and spinalis
muscles. This group is the chief extensor of the vertebral column.
These three muscles occupy the area between the spinous processes
centrally and the angles of the ribs laterally. They are ordered
lateral to medial: the iliocostalis forms the lateral column, the
longissimus forms the intermediate column, and the spinalis forms the
medial column. Each column is divided regionally into three parts
according to the superior attachments: iliocostalis is subdivided into
the cervicis, thoracis and lumborum; the longissimus and spinalis are
subdivided into the capitis, cervicis, and thoracic portions.
Deep layer of intrinsic back muscles also known as transversospinal
muscle group, and include semispinalis, multifidus, and rotatores
muscles
(Picture 6)
As all transversospinalis mucles have
common origins and insertions, the muscle layers are difficult to
accurately separate from each other. They are much shorter muscles,
situated deep to the erector spinae, and run obliquely. These muscles
originate from transverse processes of vertebrae and pass to spinous
processes of more superior vertebrae. They occupy the valley between
the transverse and the spinous processes.
The semispinalis is the superficial member of the group. It is divided
into three parts
according to the superior attachments: semispinalis capitis,
semispinalis thoracis, and semispinalis cervicis.
The multifidus is the
middle layer of the group and consists of short, triangular muscular
bundles that are thickest in the lumbar region.
The rotatores are the
deepest of the three layers of transversospinal muscles and are best
developed in the thoracic region.
As it is stated above, the deep back muscles can be grouped into
superficial, intermediate,
and deep layers. However, there is also another group, which can be
classified as minor deep layer muscles.
These are: The
interspinal (connects spinous processes), intertransverse (connects
transverse processes), and elevators of ribs (represent the posterior
intertransverse muscles of the neck) are minor deep back muscles that
are poorly developed in the thoracic region.
Anterior spinal muscles
Other than all those
abovementioned back muscles, there are anterior spinal muscles. The
anterior musculature is found in the cervical and lumbar regions, not
in the thoracic region. Namely, these are longus colli, capitis,
quadratus lumborum and psoas muscles. These are function as spine
stabilizers. Some muscles of the body do not attach to the spinal
column directly but play a role in spinal stability and motion
(abdominal muscles) or in pelvic stabilization forming a stable base
for the spine (glutei and hamstrings).
Any comment about this page?
Your feedback is appreciated. Please click
here.
Follow & Share
Scientific Spine
To join
Scientific Spine mailing list,
click here.